What Healthcare Measurement and Improvement Has Become, And What it Could Be

This is a guest post from Southcentral Foundation Senior Medical Director Dr. Steve Tierney. This article was first published on October 29, 2018 on LinkedIn.
Medicine used to be a discipline for heroes. Doctors and nurses were these heroic self-sacrificing figures who went without food, sleep, personal comforts and any hope of a normal work-life balance. They dedicated their lives (and often unwittingly their families’ lives) to the service and sacrifice of the practice of medicine. They were pillars of the communities they lived in, respected for the work they did. Then came “healthcare.”
The new age dawned with the now iconic Quality Chasm publication. We realized our heroes were not as perfect as they had seemed. The grace we gave them for the sacrifices they made was starkly revealed in the harsh cold light of data. The truth is there were mistakes being made. People were being injured. We needed a plan to somehow turn the tide. And then there was Edward Deming.
The quality journey began in the places where the most obvious events were occurring, the hospitals. What Deming brought was a systematic approach. Using his legacy work with the auto industry, we added process where before there was none. Adding structure in settings where there wasn’t any added a method to try, test and review what was happening using measurement. The ship started to turn. Infections went down; surgeries had fewer complications. Around this new period of introspection, the anesthesia specialists integrated lessons from the airline industry about standardization and process. “Healthcare” was becoming more than the practice of medicine as a self-deprecating sacrifice, but instead an industry that measured itself using process and outcome. The lamp had been lit. Armies of healthcare quality organizations and regulators were born. Being certified by the proper oversight organizations became critical to survive in this new quality-oriented healthcare industry. Gone were the days of the hero doctors. They had been replaced by certified quality organizations and scorecards with ratings. The definitions were now being set externally, using standardization and process. Then came the Electronic Health Record.
Suddenly with the new age EHR’s, all this process information was becoming easier to collect. Health plans, insurance companies, and regulators all wanted to set the standards for the best approach for each event of care. In some settings, this made work much easier. When ordering a ventilator bundle, a central line, or even chest pain protocols, it became easier to standardize what was being done. Since there were only a few EHR’s that met all of the certification requirements for use, they dictated the workflow for executing these standardized approaches to care. Quality was now being defined by process and measured by what was documented in the chart. Standards were being met. With only a few EHR’s, work was looking the same across many sites. The industry was becoming a Deming dream of standardized process. Soon, our charts were the healthiest they had ever been. One problem: Were the people as healthy as their charts? If it was not documented, was it not done or not known?
For “events” of care, the healthcare industry was becoming more standardized with what it did for charting and how it did it. For total knee replacements or bypass surgery, standardization resulted in a match between what happened to the people and what was written in the chart. But was this also the case in ambulatory settings where care was more longitudinal over time as opposed to an isolated event?
Something else was happening. Healthcare professionals were experiencing burnout. Job satisfaction and turnover were up. How did we go from heroes routinely working 65 hours a week with high job satisfaction and community respect to burned out, dissatisfied staff who typically worked fewer hours each week? How did we go from being pillars of our communities recognized for our dedication and sacrifice to having our lives summed up by 3 reviews online with Health Grades? What had shifted?
I believe in our zeal to define each care event and impose one-size-fits-all “best practice” definitions with quality defined by what was written in the chart, we overreached. We assumed all sites had the same resources, revenue streams and populations. In some settings, there clearly was an answer for the established way to best handle a central line or ventilator, but is there a best practice way to handle a longitudinal relationship? To speak with someone about life change?
When you partner with someone around a chronic condition or attempt to help them address a lifestyle or external socioeconomic pressure, is there a standard way? How much value is added when you give another copy of a printout about diabetes to someone who you have worked with for 25 years and who has perfectly controlled measured results? As if this wasn’t complex enough, suddenly enter Social Determinants of Health.
We had correctly realized that socioeconomic factors played a big role, but we had incorrectly identified both a total knee replacement and an office visit as “events” of care. While one was a fixed point in time with a clear beginning and end, and the other was a longitudinal relationship. Where a knee replacement is applied to a specific individual at a specific hour, ambulatory care is applied to entire populations over years. Have we made a big mistake? Have we confused apples with oranges? And, is it enough for a care provider to know what someone’s social determinants are? Does documenting them only add work without adding value? Can you standardize long-term relationship documentation with no clear beginning or end and apply that to an individual and simultaneously to a population?
If you haven’t guessed it, I don’t believe you can. It’s not possible. We have made a colossal mistake. One setting is a highly-controlled time-limited event with a clear start and stop applied to a person. The other is a shifting mix of changing social, economic, technological and health status variables. The documentation in the chart during these acute events can approximate the health of the person it’s applied to. In the second setting, what’s written has often very little to do with the reality for the person being attended to. It’s impossible to keep up to date. Does that mean we’re done?
Again, I say no. We just need a different way of thinking. Imagine your population is a large number of water sources and your ambulatory healthcare system is a water treatment plant. Its job is to pass all the water through and filter it – remove the impurities we might refer to as illness or risk — and to do so with a flow that allows all the water that needs to be treated in the proper amount of time. If you thought of each member of your workforce as specialized “filters,” each with its own qualities based on their training and available resources, a person receiving care should be altered by this filtration process, or another way to think about it, as they pass through (interact with) that filter. If your filters are set up with the correct qualities and in the right order for the right water source, all incoming water from all sources will be filtered in a way that makes them as equal as possible at the end of the treatment process. “Improvement” would be assessed by continually testing water quality at the end of the processing plant. If quality is less than optimal then the filtration process is rearranged or its capacity changed.
Let me be a little granular. If you assume that each of your staff will act with good intent and use the training and resources they have been given to improve the people they interact with, then as long as the post treatment water quality is continually monitored, all that needs to happen is the people being treated should interact with the correct mix of staff members. This does not prescribe how, or when or via what process for the interaction; it simply means the interaction should happen. These interactions are enough of a process as long as the overall quality output is measured. Interventions become more about augmenting the order, resources or training of those staff. Process interventions [or “requirements”] would be as limited as possible given that this environment is a continuous ongoing relationship that should be left as fluid as possible to adapt to a myriad of constantly changing variables. Limiting process steps would both increase the capacity and reduce non-value-added work (and burnout).
How is that even possible? How would you even begin? The truth is Facebook, Amazon, Twitter and Netflix do this almost constantly in real time. Using only virtual assessment and outcome review (what is watched, when and by whom) you could apply the same approach to population health. If you created a matrix for your population, with a matrix of all your available “filters” (think of each healthcare staff member as a resource) you could continuously run things like the HEDIS dashboard, ER visit rates, admission rates, readmission rates, vaccination rates, visit rates of all types, costs/person/yr, and satisfaction rates. You could then review the list of “filters” that each individual passed through and optimize “filter placement.”
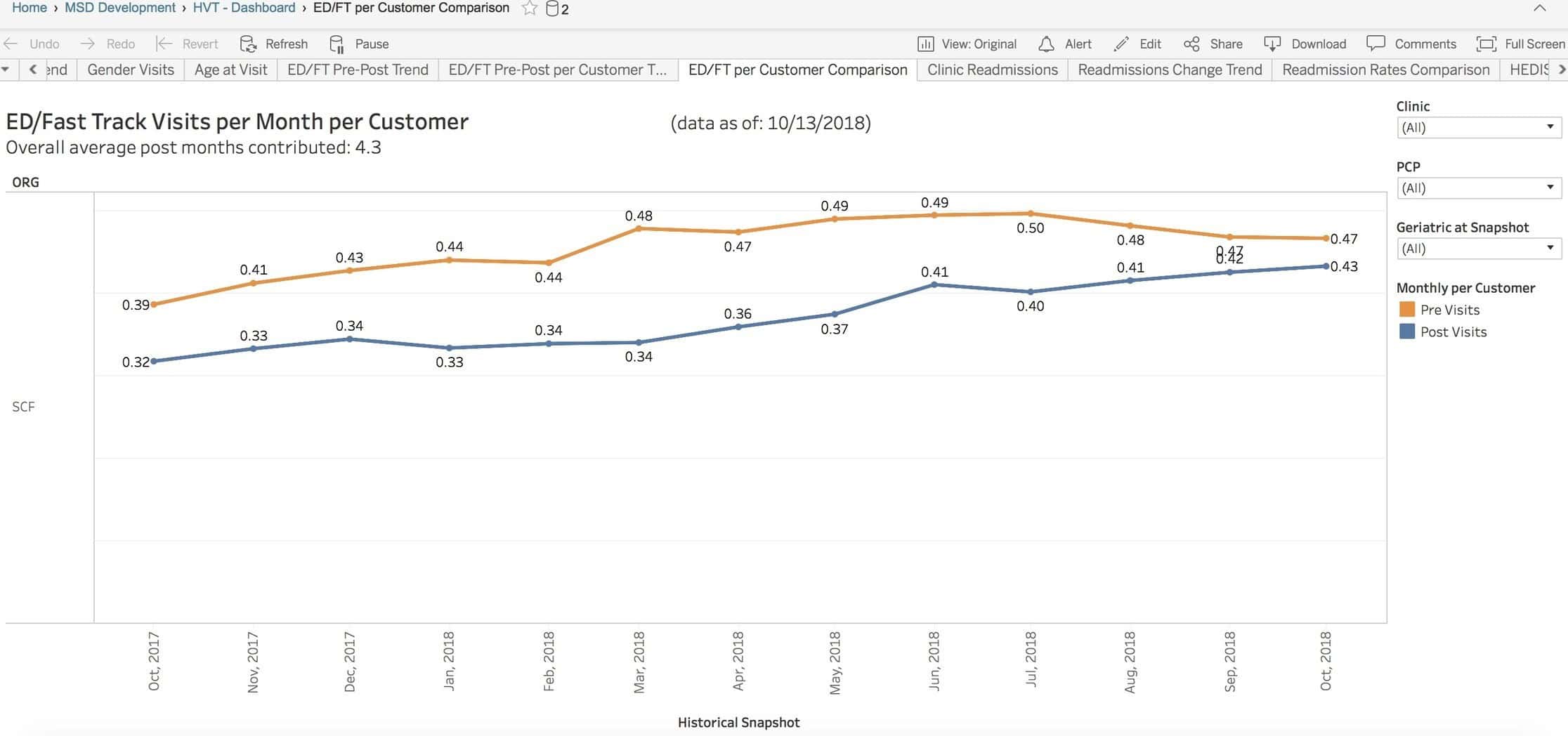
Here is an example reviewing the pre- and post-ER Visit rates after being “filtered” through a home visiting nurse resource. Notice the impact.
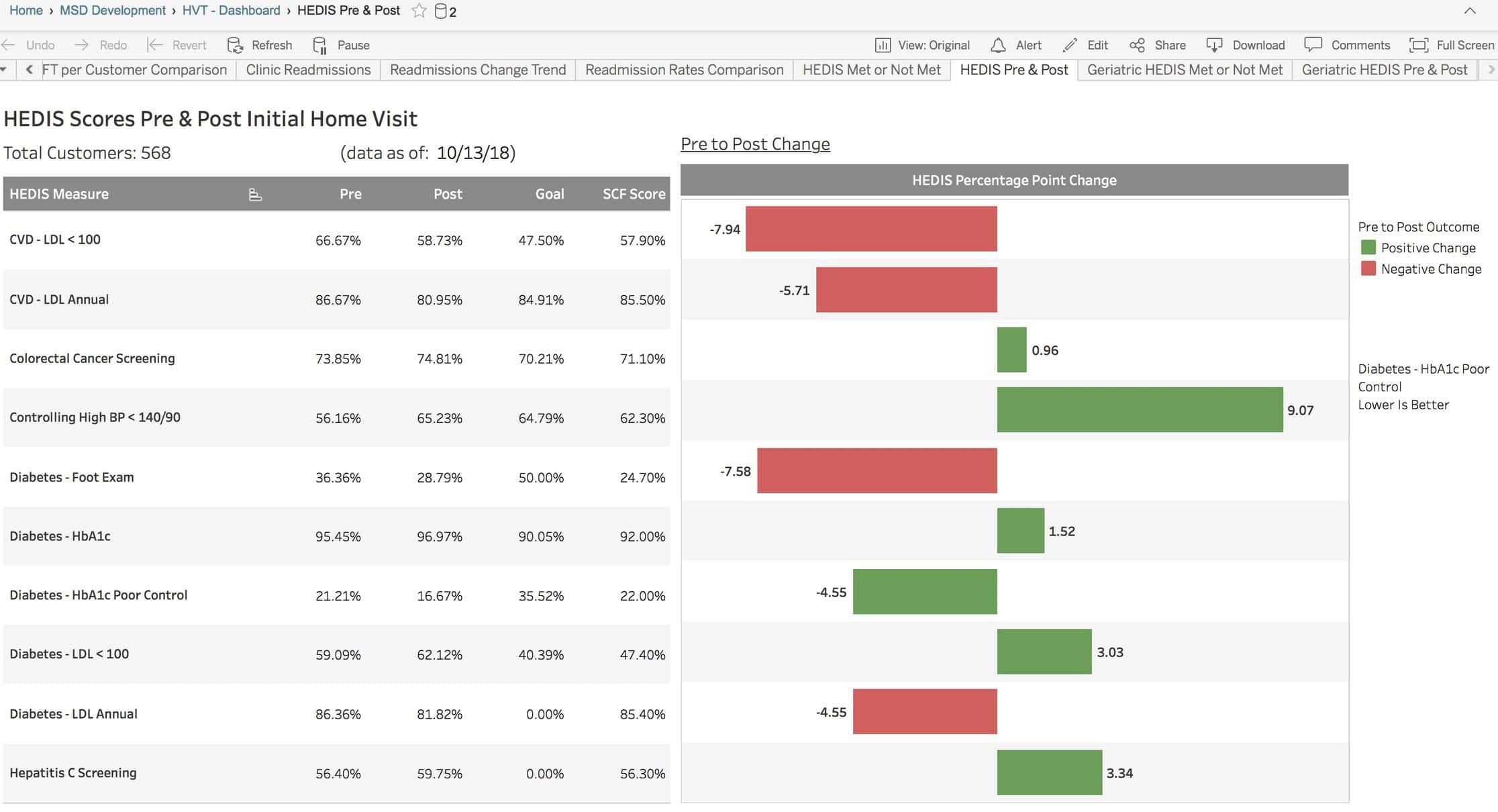
Here is another example: how the HEDIS Dashboard was impacted both pre and post the same Visiting Nurse Resource application.
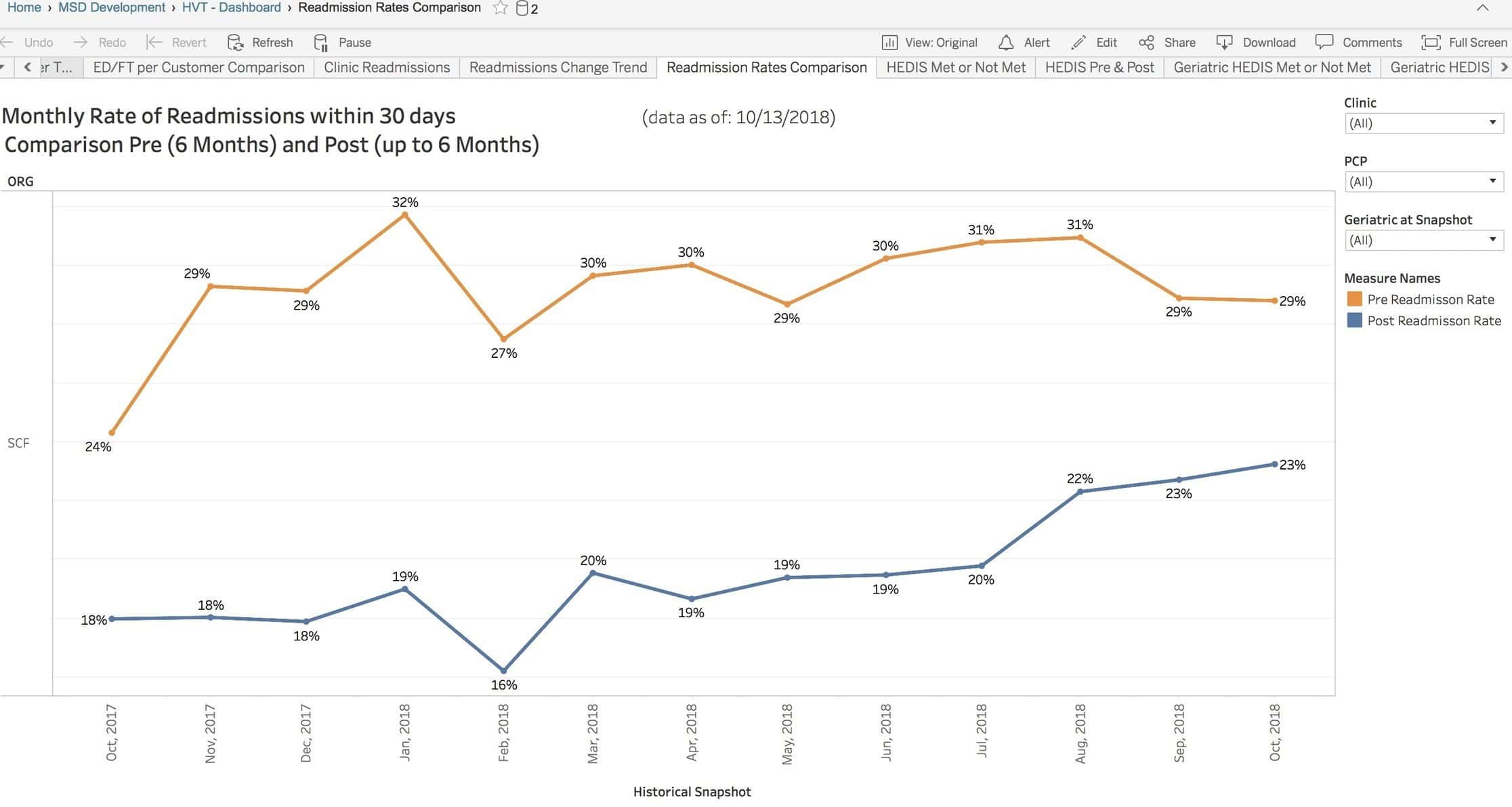
Here is the impact of the same resource on readmission rates.
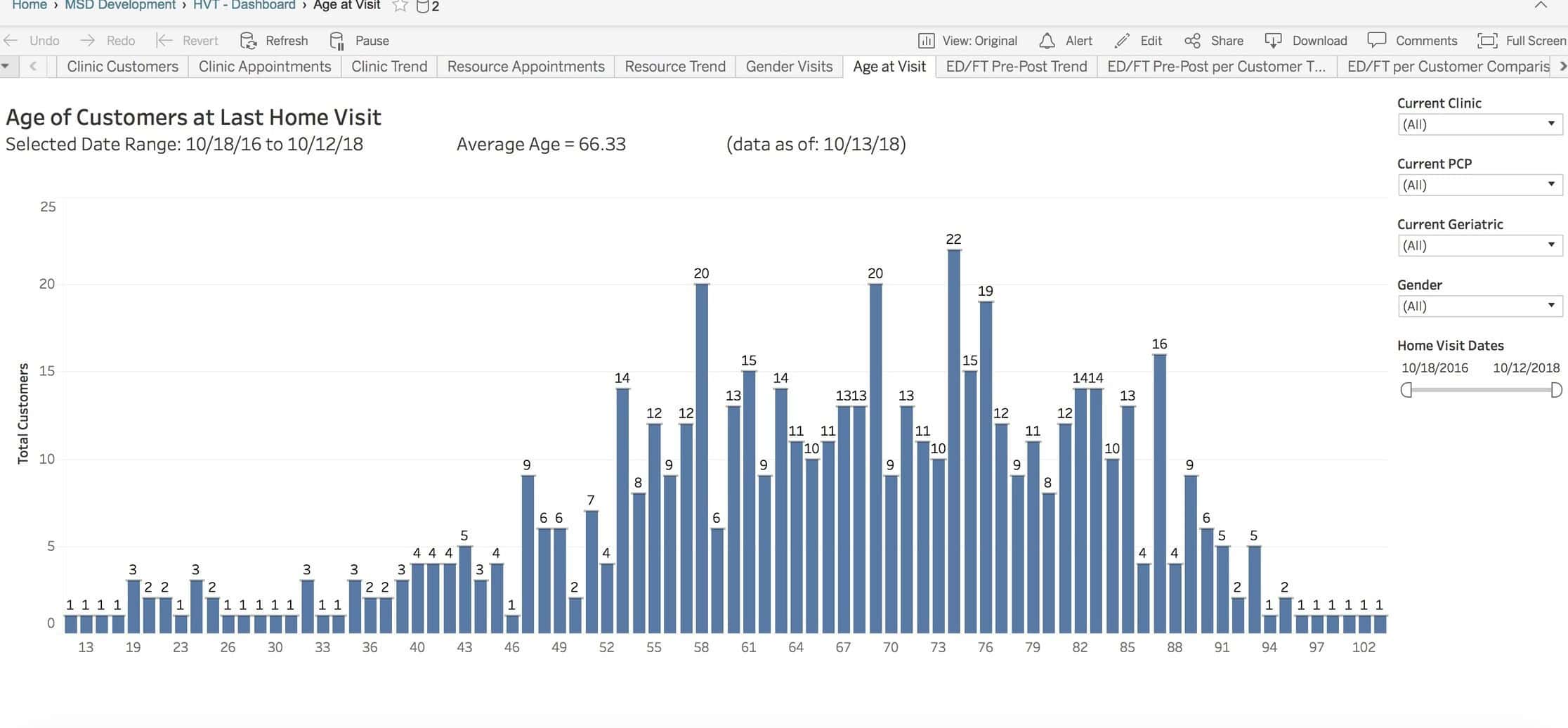
Notice the resources at the right. You can filter the view by any time range, clinic location and any resource who had an interaction with an individual (or was “filtered” by).
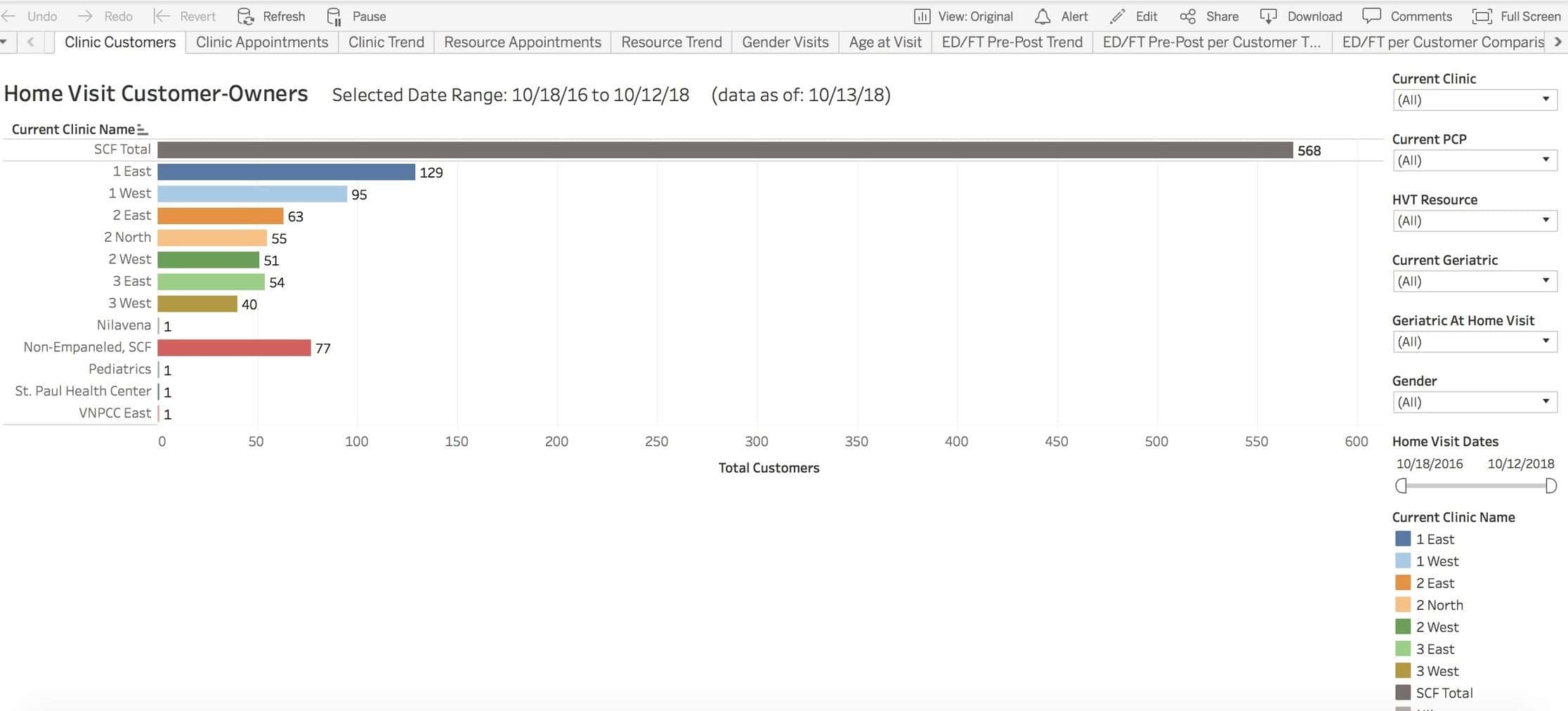
You can look at age distribution at the time of visit or any other variable like gender, zip code or individual staff member as opposed to staff member type.
This is what this means: If you get out of the way of the staff, strip all process possible, and continuously monitor (simultaneously) all individuals interacted with, as well as all resources for a wide range of criteria that anyone would agree are value added (like admissions, readmissions, ER use, vaccinations, chronic condition control, opiate use, and cancer screening to name a few), you would have a true population outcome view rather than a visit-based set of standardized behaviors. In other words, monitor everything on everybody your system cares for all the time and continuously measure the impact of any resource or resources on all items simultaneously.
Population health needs to be about the population, not the process. Acute short-term care can be improved with process, but while this type of care has a clear beginning and end, population health does not and will defy analysis by event-based parameters.
Working in teams, shifting measurement to a population-wide platform, leveraging staff members’ collective impact and adjusting workflow based on outcome, not process, has to be the new developing edge for ambulatory healthcare. Let’s stop mixing apples with oranges and pretending acute and population healthcare are the same.

